The day after Leonid's lengthy presentation at the Pacific Rim International Conference on Disabilities, we met him and Mark (ABR researcher) at the rehab department where Abbie receives her therapy. He was kind enough to meet with Abbie's entire team, who all attended the presentation the day before, to delve more deeply into certain topics, and to assess Abbie. We were even joined by her orthopedic surgeon for an hour...a stunning amount of generosity, given his very crammed schedule.
We took video of the assessement, but I have not seen it yet - so, this will be from memory. It won't be hard though, because the highlights (or lowlights) were searing to receive.
I. The Value of Stillness
Traditionally, we always look for the culprits to "retrain"..those loud, noisy, bullying muscles. If an electro-myelograph is done, the large muscles literally scream for attention so insistently that it's hard to focus on anything speaking more softly, and impossible to consider those not speaking at all.
Leonid came up with an apt analogy for this: a foreigner, previously unexposed to the USA hears only the 50 or so congresspersons who hog the media, and adds to that the input of our outspoken stars and starlets, and comes away thinking he understands the whole of what America is about. That is what we do when we figure out the body by paying attention to those parts that wail for our attention. Both views are utterly incomplete, inaccurate, and lead us to all sorts of false conclusions.
The connective tissue, on EMG, is silent, going about its tasks in the unassuming way that results in invisibility. Not only do we listen for the shouts and ignore the silent tissues, but we look for the movements. If a part of the body is not designed to move, we pay it no heed, never thinking that the stillness may be critical to overall function, and its loss a key barrier to health.
As you sit reading this, place one hand gently on your trachea (windpipe) - then, turn your head to the right and left a few times. How far out of midline did your trachea move? Not at all, right? THAT is stillness, so taken for granted that we don't even notice or appreciate it.
The support structures of Abbie's neck have collapsed so completely that her trachea moves all over the place. When her head is turned to the left, it is deviated to the right, and vice versa. The weakness in her neck is apparent once you know that bulging is an obvious sign. Because her trachea is not anchored by the connective tissue and ligaments, she prefers a head position that makes it easiest to breathe.
Think about gasping for air after a sprint. What do we naturally do during the initial recovery? We throw our heads back and gulp in the air. This is part of the reason she prefers what we call a "nose in the air" position (the other part will be explained later). So, when well-meaning people reposition her head to look straight forward at midline, she feels her airway being somewhat restricted and turns her head to the side to relieve it. I've always been told it's a neurological thing - this preference for head-turning. Yea...not so sure that's the whole picture now.
Abbie has lost the stillness not only in her neck, but at the upper parts of her thoracic cavity (chest). She is not using the upper lobes of her chest much at all, which has turned them into a "sewer". We cannot even start doing ABR on her upper chest until we get other areas strengthened in order to drain the swamp, otherwise she will be overwhelmed.
Understanding the ramifications of stillness, and its loss, made me appreciate connective tissue even more.
II. The Answer to the Secretion Challenge
Everywhere Abbie goes, her suction machine goes. Airport security absolutely stresses me out, because they insist on separating the girl from her mechanical pal -- and even 10 minutes can be too long sometimes.
It wasn't always this way. After she was decannulated, we didn't even turn it on once for 3 months, until she got a cold. Since then, our constant companion has seen progressively more use. I have wracked my brain to figure out what I am feeding her that may cause secretions. What is in the air she may be reacting to? Reflux meds made no difference. This has been one mystery that has almost driven me mad.
And then, here comes the simple answer from left field. Everyone's lungs make copious amounts (30 liters or so) of secretions each day to keep the lungs lubricated. We have the pneumatic and hydraulic pressures and capacities to pump these properly through the system. They are partially dispersed by seeping through (under pressure) from the thoracic to the abdominal cavity.
Well, Miss Abbie's pumps are no longer working, resulting in the pooling. The collapse of her tissue has made it very dense so seepage is not possible (and there isn't adequate pressure to push it right now anyway). Hence, the only way she can clear her lungs is to excrete it through her mouth and nose...often. How thankful I am, then, that she has a strong cough -- which she showed off to Mark and Leonid, resulting in a "cough zone" reminiscent of a Gallagher show.
So, much of her secretion challenge is mechanical....partially related to reflux caused by weakness (I think), and partially related to the "extreme weakness" of her respiratory system.
Those words in quotes were hard for me to hear, as I have felt it coming, but didn't know how far she had sunk.
Leonid had us get on one side of Abbie as she was lying on her back, and then reach to the far side of her chest with both our hands. We compressed her chest with both hands, and it folded like fragile butterfly wings. My throat clamped shut and tears came.
Her ribs are no longer oriented parallel to the ground, but are more vertical, so that as force comes up from the ground as she is sitting, she doesn't have the mechanical structure to handle and distribute the force properly. It's like injury on top of insult on top of impossibility...
Later that evening I overheard Leonid tell someone that Abbie's respiratory system is "hanging on by a thread." Ugh.
III. Fake Versus Real
Leonid sat Abbie at the edge of the massage table and held her at the bottom of her ribs. She was sitting pretty well, and we were happy with that....for just a second. Then he pronounced, "This is fake."
She was not using strength to hold herself up, but rather was relying on a restriction in her lumbar spine that prevents her from falling forward. Great...so all this progress we had been seeing in this area was only her tapping more deeply into the inflexibility of her spine. Useful, smart...damaging.
It's a great way to keep her from face-planting when seated, but as the restriction deepens through use it pulls down on the back of her skull -- the other factor in her "nose-up" preference. As the downward pull has been tilting her head back, her jaw assumed a more open position. So much so, in fact, that location of her of molars drifted so that currently, even if she wants to close her mouth, she can't because her back teeth meet before her mouth closes.
The more we practice sitting with her, the more we enhance the fake and prevent real strength. What a conundrum. He made sure we realized that as we progress through the ABR process, there will come a time when that restriction releases, but strength has not been built up yet. In other words, there will be days of face-planting. Never thought I would look forward to that, but I do now.
The whole "fake versus real" issue looms large when we think about little ones who may have been born with challenges. A mother's intuition may be prodding her, telling her something is not right. But, if her baby "meets milestones" in reasonable amounts of time, she is told her child will be OK.
But, what if a child is holding his head up via a restriction or spasticity (fake) instead of strength (real). What if instead of rolling (real) he is flipping (fake)? These differences take trained attention and the right paradigm to notice, but ignoring them allows a child's challenges to slip by under the radar until perhaps years of opportunity have drifted by.
I acutely felt the loss of those years when, later that evening, Leonid saw a large photo of Abbie on our piano. "How long ago was that taken?" He asked.
Hmmmm..I had to think for a moment....three years.
"Wow -- look how much better she looked back then," he said.
Ouch. The truth stung hard.
Pulled down by the head tilt and let go by the tissue collapse, her face has seemingly slid down her skull...her cheeks are smaller and her jowls are bigger. It is harder for her to smile. I did see all this happening, bit by bit, and I felt helpless to stop it.
It's strange to be sad as I look pictures of her as a four-year-old. It used to be that only pre-drowning photos could stab my heart. But, now I see how far she has gone in the wrong direction from those early years. Oh, I wish I had known what I know now.....but I remain thankful that I have learned in time to help her.
There is even more we learned, but I will save that for another post, as I have to go, and I'm sure you do, too.
Just one little "Abbie-ism" I have to share first. The day of evaluation was all about "weakness, extreme weakness, and profound weakness" all over Abbie's body. At bedtime that night I could tell she was distressed, and took a chance that I knew what it was.
"Abbie -- I know that today everyone kept saying over and over how weak you are. But, you know what? You are strong where it counts! Everything else can be fixed, but you are strong in your heart, and in your spirit and that is what matters."
A smile came, and sleep followed soon after.
She always has been, and remains....strong where it counts.
Tuesday, May 10, 2011
Thursday, May 05, 2011
ABR 2: Stress Shielding and the Vicious Cycle
As we begin to make the mental shift from force generation (muscles) to force transfer (connective tissue) as a target for therapeutic interventions, one of the first things we need to realize is that the body of a brain-injured person, or pa erson with CP, is a mix of strong and weak tissues, often in combinations that boggle the mind.
Traditionally, we have been obsessed with the strong, bullying tissues. We give medications to relax them, do surgery to release them, inject Botox to paralyze them, but never really give a thought to the other side of the coin. How do we strengthen the weak tissues? I envision it at somewhat like the challenges in classrooms today. Do we keep the class moving along together by holding back the bright children (easy) or strengthening the challenged learners (difficult)?
We've focused on the strong partially because we have had no means to strengthen the weak. ABR gives us this opportunity, but it doesn't mean the strong tissues are going to give up without resistance. In fact, they have become so adept at their roles, which in some cases are helpful to the person although ultimately destructive (like the high muscle tone that may help a child sit, but will eventually contort the spine), that we must sneak past them to build up the weak tissues.
This is a rough picture of something called "Stress Shielding", where the strong tissues absorb incoming mechanical stresses to protect the weaker tissues, and in the process become even stronger while the weak tissues continue their decline fomented by neglect.
In a normal body, there is a cycle of tissue remodeling that looks like this, what Leonid has termed "The Virtuous (Sustainable) Cycle":
 This cycle can continue in a positive, healthy way because when mechanical stress enters the body it is sustainably and efficiently distribute by and between tissues that are balanced. This well-distributed stress is then used to maintain the vitality of the tissues appropriately, so that the cycle can continue.
This cycle can continue in a positive, healthy way because when mechanical stress enters the body it is sustainably and efficiently distribute by and between tissues that are balanced. This well-distributed stress is then used to maintain the vitality of the tissues appropriately, so that the cycle can continue.
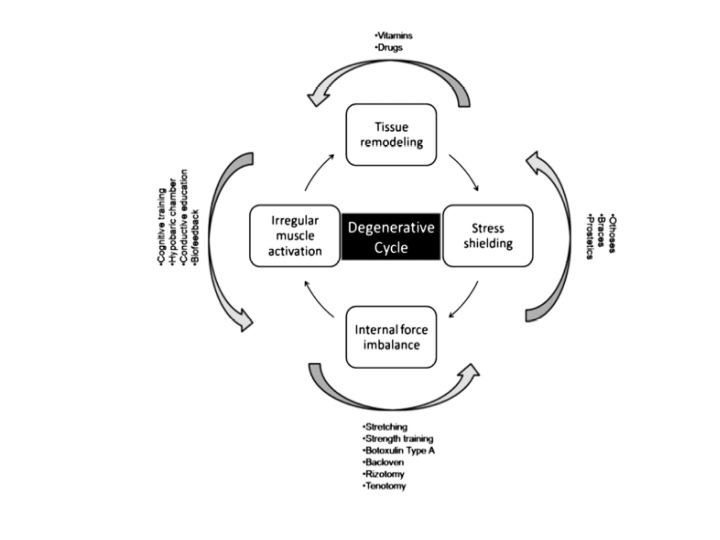
In a person whose tissue are a mix of strong and weak, the cycle looks like this:

I know the words on the outside of the circle are hard to read, but they are the lists of interventions that are typically applied to counteract the negatives at each of the stations of the circle. Usually, they are of little to no avail in moderately to severely impacted people, and so their movement through the vicious cycle continues.
You can jump in at any point on the circle and envision what happens. Say that you start at "irregular muscle activation" -- this pattern of use leads to tissue remodeling that reinforces this negative pattern...reinforcing the underlying mix of strong and weak. With the tissue differentiated this way, stress shielding kicks in, as the strong absorb the lion's share of mechanical stress, and deprive weak tissue of the stress they need to get stronger. The disparities between the tissues lead to internal force imbalances, with the strong tissues being strengthened even more by the imbalance. This leads us right back to irregular muscle activation.
Look, many physically disabled people have a very high "Motor IQ"...being so limited they are endlessly creative and persistent in finding a way, any way, to make their bodies accomplish what they desire. If "irregular muscle activation" allows them to use a communication device or control a power chair, it's very difficult to say , "Hey, try not to use your body in that way -- it's a destructive pattern."
But, we are not just talking about voluntary muscles, we are talking about all tissues, so halting this destructive cycle is not about "retraining muscle movement". It is ongoing 24/7, even as a person is apparently still, or even sleeping. The only way to reverse it is by strengthening the weak tissue, to balance the force distribution and negate the stress shielding response.
A good visual analogy of stress shielding is to align a length of steel cable next to an equivalent length of rubber band. As you stretch them together, you know that they will only reach the length of the steel cable, which will be absorbing all of the stress. The only way to introduce stress to the rubber band is to work around (without) the cable.
How can we do this in the body? Our first instinct, when trying to provide mechanical stress to deep fascia, is to press harder, to make sure the stress reaches far enough. All we are doing with this approach is activating the stress shielding response and strengthening the strong.
We have to go gently in --- so gently that the movement is almost imperceptible. It truly is like sneaking in under a wire. ABR aims for a 1-2% deformation of underlying tissue. To compare, range of motion exercises and fascial release generally aim for 3-8% deformation. Beside activation of stress shielding, there are a couple of other challenges with this higher range.
Tissue deformation at 3-8% is the introduction of microtrauma to the tissues. This is how healthy people get stronger. When we push ourselves at the gym, our muscles respond to the microtrauma by getting stronger over time. But, recall that people in the moderate to severe range of impact are metabolically broke -- they can't afford to fix microtraumas, especially not on a daily basis (as range of motion is often prescribed) and in many areas simultaneously.
Secondly, to achieve gains from range of motion exercises, they must be applied to the very end of the range. This gets rather technical and challenging, and is a skill difficult to easily and effectively transfer into the hands of parents and caregivers.
So, ABR provides a fortunate confluence of variables: the 1-2% deformation of tissue sneaks past stress-shielding, doesn't induce physically-expensive microtrauma, and can be safely accomplished by lay people. And yes, this small window also means that it takes time and repetition. ABR is not a quick fix, not even a moderately-fast fix. It is a long-term, one small step at a time approach.
But hey, our brain injured loved ones are never standing still...they are either getting better or worse each day. So, I am more than happy to take small steps, as long as I know they are in the right direction.
I know this was a really long posting....now that I've given you the "why" of the ABR technique, tomorrow I will delve more deeply into the "how"
Traditionally, we have been obsessed with the strong, bullying tissues. We give medications to relax them, do surgery to release them, inject Botox to paralyze them, but never really give a thought to the other side of the coin. How do we strengthen the weak tissues? I envision it at somewhat like the challenges in classrooms today. Do we keep the class moving along together by holding back the bright children (easy) or strengthening the challenged learners (difficult)?
We've focused on the strong partially because we have had no means to strengthen the weak. ABR gives us this opportunity, but it doesn't mean the strong tissues are going to give up without resistance. In fact, they have become so adept at their roles, which in some cases are helpful to the person although ultimately destructive (like the high muscle tone that may help a child sit, but will eventually contort the spine), that we must sneak past them to build up the weak tissues.
This is a rough picture of something called "Stress Shielding", where the strong tissues absorb incoming mechanical stresses to protect the weaker tissues, and in the process become even stronger while the weak tissues continue their decline fomented by neglect.
In a normal body, there is a cycle of tissue remodeling that looks like this, what Leonid has termed "The Virtuous (Sustainable) Cycle":

In a person whose tissue are a mix of strong and weak, the cycle looks like this:
I know the words on the outside of the circle are hard to read, but they are the lists of interventions that are typically applied to counteract the negatives at each of the stations of the circle. Usually, they are of little to no avail in moderately to severely impacted people, and so their movement through the vicious cycle continues.
You can jump in at any point on the circle and envision what happens. Say that you start at "irregular muscle activation" -- this pattern of use leads to tissue remodeling that reinforces this negative pattern...reinforcing the underlying mix of strong and weak. With the tissue differentiated this way, stress shielding kicks in, as the strong absorb the lion's share of mechanical stress, and deprive weak tissue of the stress they need to get stronger. The disparities between the tissues lead to internal force imbalances, with the strong tissues being strengthened even more by the imbalance. This leads us right back to irregular muscle activation.
Look, many physically disabled people have a very high "Motor IQ"...being so limited they are endlessly creative and persistent in finding a way, any way, to make their bodies accomplish what they desire. If "irregular muscle activation" allows them to use a communication device or control a power chair, it's very difficult to say , "Hey, try not to use your body in that way -- it's a destructive pattern."
But, we are not just talking about voluntary muscles, we are talking about all tissues, so halting this destructive cycle is not about "retraining muscle movement". It is ongoing 24/7, even as a person is apparently still, or even sleeping. The only way to reverse it is by strengthening the weak tissue, to balance the force distribution and negate the stress shielding response.
A good visual analogy of stress shielding is to align a length of steel cable next to an equivalent length of rubber band. As you stretch them together, you know that they will only reach the length of the steel cable, which will be absorbing all of the stress. The only way to introduce stress to the rubber band is to work around (without) the cable.
How can we do this in the body? Our first instinct, when trying to provide mechanical stress to deep fascia, is to press harder, to make sure the stress reaches far enough. All we are doing with this approach is activating the stress shielding response and strengthening the strong.
We have to go gently in --- so gently that the movement is almost imperceptible. It truly is like sneaking in under a wire. ABR aims for a 1-2% deformation of underlying tissue. To compare, range of motion exercises and fascial release generally aim for 3-8% deformation. Beside activation of stress shielding, there are a couple of other challenges with this higher range.
Tissue deformation at 3-8% is the introduction of microtrauma to the tissues. This is how healthy people get stronger. When we push ourselves at the gym, our muscles respond to the microtrauma by getting stronger over time. But, recall that people in the moderate to severe range of impact are metabolically broke -- they can't afford to fix microtraumas, especially not on a daily basis (as range of motion is often prescribed) and in many areas simultaneously.
Secondly, to achieve gains from range of motion exercises, they must be applied to the very end of the range. This gets rather technical and challenging, and is a skill difficult to easily and effectively transfer into the hands of parents and caregivers.
So, ABR provides a fortunate confluence of variables: the 1-2% deformation of tissue sneaks past stress-shielding, doesn't induce physically-expensive microtrauma, and can be safely accomplished by lay people. And yes, this small window also means that it takes time and repetition. ABR is not a quick fix, not even a moderately-fast fix. It is a long-term, one small step at a time approach.
But hey, our brain injured loved ones are never standing still...they are either getting better or worse each day. So, I am more than happy to take small steps, as long as I know they are in the right direction.
I know this was a really long posting....now that I've given you the "why" of the ABR technique, tomorrow I will delve more deeply into the "how"
Monday, May 02, 2011
ABR 1: Lavish versus Thrifty
In researching ABR I watched hours of video, piecing together the theory and application as best I could. It was a great relief when Leonid, while visiting Hawaii, framed it in a way that made it immediately relevant and clear. He introduced us to the concept of “Lavish” versus “Thrifty” rehabilitation.

As you can see, "Level 1" is the least affected, while "Level 5" is the most affected. Lavish methods may be effective for Levels 1 and 2, but for Levels 3, 4, and 5 they are increasingly less effective. It is often tempting, after seeing progress in a Level 1 or 2 person, to replicate the approach in a Level 3, 4 or 5 person, while thinking, "Well, we may not achieve as much, but at least we may gain something."
Unfortunately, since the lavish approach bankrupts the Level 3, 4 and 5 people, not only do they not achieve gains, but they make things worse.
The collapse of the connective tissue has great impact on the respiratory system, the digestive system, as well as posture. I can tell you that every parent of a spastic quad child is dealing with challenges in all these areas. Normally we are given medications (nebulizers, inhalers, anti-secretion, anti-reflux, digestive motility aides, anti-spasticity) and all manner of splints, braces and supports. What we are not given, unfortunately, are solutions. Our children continue their declines at rates that seem to accelerate over time.
I sit here typing on the first Monday in May....the day Abbie drowned seven years ago. Through these challenging years I have often comforted myself by saying, "My daughter is not an oncology patient. I am not beating back something trying to kill her." But, in the last six months, I have realized that comfort is an illusion. She is dying, more rapidly each day, as her respiratory system begins to cave under increasing strain.
Leonid's in-depth evaluation, which I will describe in a separate post, was exquisitely painful for me, as he confirmed my fears, and shone a bright light on things I'd only seen as shadows. I try not to regret only learning about all of this now, avoiding thinking about the beautiful, strong body that has disintegrated over these years. It will be a long road out of this valley in which we find ourselves, but we are walking anyway....only, now I have confidence that perhaps we can change the direction.
More to come on typical results of connective tissue collapse, how to strengthen it, and the physical barriers we have to work around.
The most expensive things in the body are the muscles and the nervous system. They require a lot of effort to use, and the body expends a lot of metabolic energy to meet their demands. Most traditional rehabilitation focuses on one or the other, or both simultaneously as therapists, parents and aides attempt to stretch and “retrain” muscles, and give sensory and cognitive input in hopes of eliciting output.
A healthy person has adequate reserves to meet the needs of the muscles and nervous system. Some injured people also maintain enough of a metabolic “bank account” to write the energy checks these systems demand. But, in the case of the most injured people, a systemic collapse has drained their reserves, and they are unable to meet the demands of these expensive systems.
So, asking a very injured person to use the most expensive means is analogous to asking a girl without money to buy rice, to purchase steak in order to recover. Not only is it not feasible, but the attempts to use the expensive systems leave an injured person in deeper debt, in worse shape in many ways.
The connective tissue of the body, on the other hand, is extremely cheap, or "thrifty". It makes almost no metabolic demands on the body, nor any cognitive demands. It is ubiquitous - found everywhere in the body. It covers, and actually invests itself, into bones, muscles, and organs. It is the major support structure within the body. It is also completely passive, very unlike the contractile properties of muscles. So, it requires a mental shift to begin considering how to strengthen connective tissue.
To begin this shift, we can observe what happens when it collapses. A healthy person has two major "balloons" supporting her core, one in the chest and one in the abdomen. Those balloons are contained by (or even created by) connective tissue. When a person is subjected to a significant neurological trauma (either in utero or after birth at some point), the connective tissue begins to collapse.
[Side note: the thoughts within these brackets are mine, not Leonid's. Not sure if he would agree or not. Many have asked me "Why does it collapse? The first factor, I believe, is hormonal. Cortisol is a stress hormone, which destroys connective tissue after prolonged, elevated exposure. After brain injury, typically a person's cortisol levels go through the roof. Abbie's were still extremely elevated two years after her injury. There a not any really good ways to bring cortisol levels down, although DHEA supplementation can help. I have chosen not to give DHEA to Abbie at this point, because she is still pre-adolescent, but she does get pregnenolone.
The second factor is a vicious cycle. Tissues remain strong and vital by being stressed mechanically -- by moving and bearing weight. As a brain-injured person becomes locked up by spasticity, healthy biomechanical stresses become difficult to provide. Tissues weaken, fluids stagnate, and the entire system begins a gradual but steady decline. When the tissues weaken, the balloons of support act just like balloons that have been pricked, slowly losing the pneumatic pressure needed to support the core of a person.]
Once the balloons of support collapse, all the joints begin to move into the wrong places. Stepping back for a moment and realizing this makes the arrogance of our "movement retraining" approach apparent. Once a body is contorted, the person lives in what Leonid calls the "proprioceptive jungle" (proprioception is how the body perceives it's position in space and movement). Because joints are not in the proper places, nor functioning normally, the input given is altered.
We, on the other hand, blessed with healthy bodies and normal proprioceptive capabilities are "urban dwellers". We then approach the jungle dwellers and attempt to teach them how to hunt in the jungle. Just because we know from our experience how a shoulder "should" work, we think that helping a jungle dweller is as simple as forcing his shoulder to work the same way, through stretching, assisted movement, and medications. Helping a starving native tribe by telling them to google "gardening tips" makes about as much sense.
In the weeks and months after a brain injury, much investment is made in the lavish methods of rehabilitation. For those fortunate enough to have the resources to utilize these investments, recover comes in differing stages and depths. However, for those not so fortunate, the lavish efforts produce nothing worthy of comment nor celebration while in the meantime, the connective tissue collapse pushes them further from health. This points to the need to differentiate between degrees of injury -- "brain injury" is far too broad of a stroke to adequately address the varying needs.
The graph below was produced by a group in Hamilton, Ontario Canada who followed children with Cerebral Palsy for 21 years to see what levels of motor function they were able to achieve. Although this is geared for CP, I think it is instructive when we talk about motor recovery in brain injury in general.
The graph below was produced by a group in Hamilton, Ontario Canada who followed children with Cerebral Palsy for 21 years to see what levels of motor function they were able to achieve. Although this is geared for CP, I think it is instructive when we talk about motor recovery in brain injury in general.
Prognosis for gross motor function in cerebral palsy: Creation of motor development curves. Journal of the American Medical Association, 288 (11), 1357-1363 Rosenbaum, P., Walter, S., Hanna, S., Palisano, R., Russell, D., Raina, P., Wood, E., Bartlett, D., & Galuppi, B. (2002).
As you can see, "Level 1" is the least affected, while "Level 5" is the most affected. Lavish methods may be effective for Levels 1 and 2, but for Levels 3, 4, and 5 they are increasingly less effective. It is often tempting, after seeing progress in a Level 1 or 2 person, to replicate the approach in a Level 3, 4 or 5 person, while thinking, "Well, we may not achieve as much, but at least we may gain something."
Unfortunately, since the lavish approach bankrupts the Level 3, 4 and 5 people, not only do they not achieve gains, but they make things worse.
The collapse of the connective tissue has great impact on the respiratory system, the digestive system, as well as posture. I can tell you that every parent of a spastic quad child is dealing with challenges in all these areas. Normally we are given medications (nebulizers, inhalers, anti-secretion, anti-reflux, digestive motility aides, anti-spasticity) and all manner of splints, braces and supports. What we are not given, unfortunately, are solutions. Our children continue their declines at rates that seem to accelerate over time.
I sit here typing on the first Monday in May....the day Abbie drowned seven years ago. Through these challenging years I have often comforted myself by saying, "My daughter is not an oncology patient. I am not beating back something trying to kill her." But, in the last six months, I have realized that comfort is an illusion. She is dying, more rapidly each day, as her respiratory system begins to cave under increasing strain.
Leonid's in-depth evaluation, which I will describe in a separate post, was exquisitely painful for me, as he confirmed my fears, and shone a bright light on things I'd only seen as shadows. I try not to regret only learning about all of this now, avoiding thinking about the beautiful, strong body that has disintegrated over these years. It will be a long road out of this valley in which we find ourselves, but we are walking anyway....only, now I have confidence that perhaps we can change the direction.
More to come on typical results of connective tissue collapse, how to strengthen it, and the physical barriers we have to work around.
Subscribe to:
Posts (Atom)